
A Practical Internal Audit Framework That Protects Agencies From Compliance Risk and Improves Clinical Quality
The documentation audit is the most powerful quality assurance tool available to home health agencies — and one of the most consistently underutilized. While most Medicare-certified home health agencies have QAPI programs that track aggregate quality metrics, far fewer have systematic internal documentation audit processes that examine the clinical record at the level of specificity where the compliance risks and quality gaps most commonly reside. The agencies that build robust internal audit programs discover their own documentation vulnerabilities before surveyors, auditors, or Recovery Audit Contractors do — and they correct them while the correction is operationally straightforward rather than legally consequential.
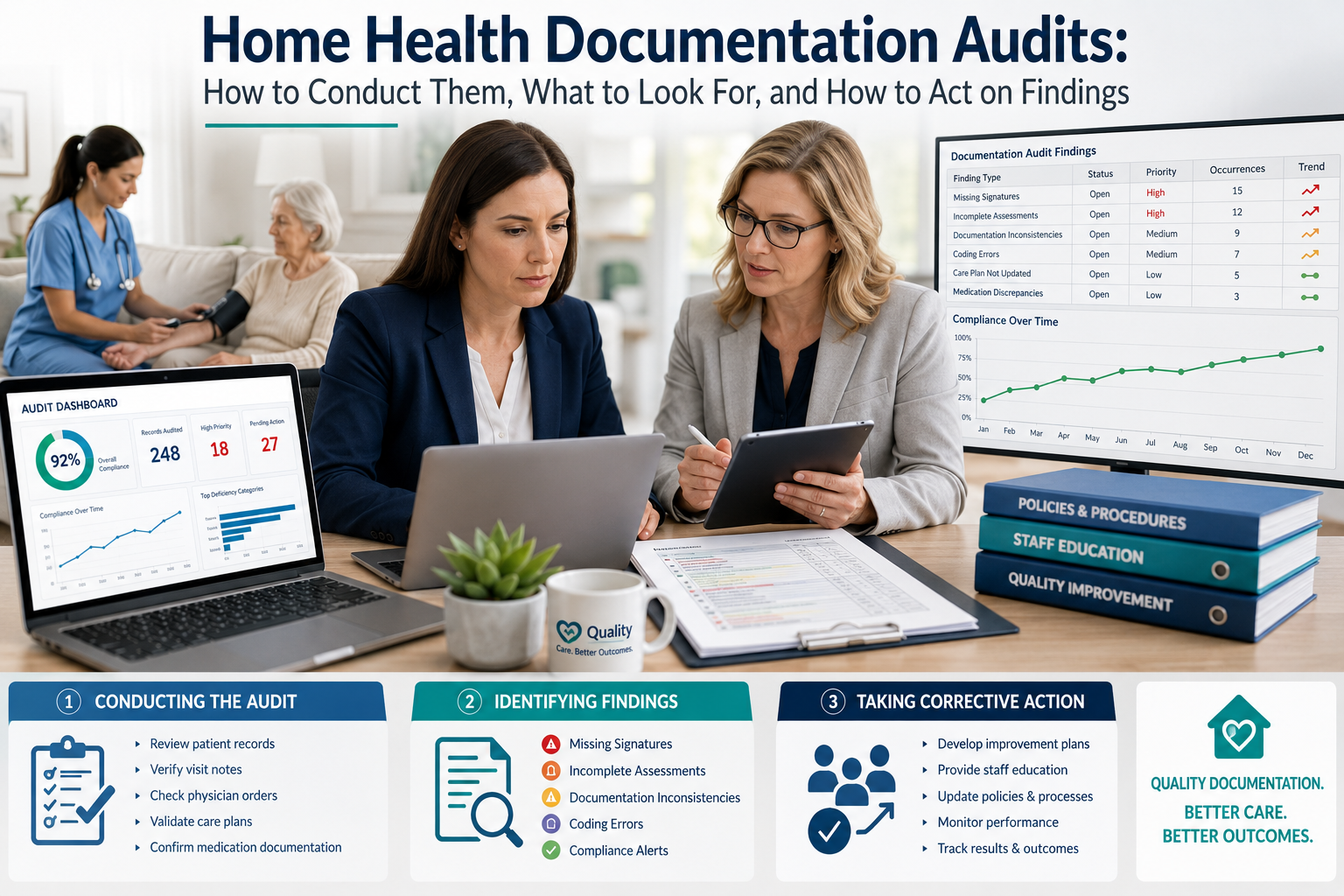
A documentation audit program begins with clarity about what it is auditing and why. The most productive audit framework distinguishes between three audit types, each serving a different purpose: prospective audits conducted during active episodes to identify and correct documentation deficiencies before billing; retrospective audits conducted on completed episodes to identify patterns and inform training; and focused audits targeting specific documentation elements where prior surveys, audits, or internal monitoring have identified elevated risk. Each type requires different sampling approaches, different review criteria, and different response processes.
Homebound status documentation is consistently among the most commonly cited compliance failures in home health, and it should be an audit priority for every agency. The homebound standard requires that leaving the home requires a considerable and taxing effort, and that when the patient does leave, it is infrequently and for durations or purposes such as medical appointments or religious services. The documentation that establishes homebound status must be specific and functional — not generic. “Patient is homebound due to multiple diagnoses” fails to meet the documentation standard. “Patient ambulates 15-20 feet with rolling walker and standby assistance; becomes significantly short of breath requiring 10-minute rest; cannot safely manage exterior steps without maximum assistance of one person” meets it. Auditors examining homebound documentation are looking for specific functional observations, not diagnostic labels.
Medical necessity documentation — establishing that skilled services are reasonable and necessary for the treatment of the patient’s condition — is the second foundational compliance documentation element that audits should systematically examine. The audit question for medical necessity is not whether the patient needs care, but whether the documentation establishes that the care being provided requires the skill, knowledge, and judgment of a licensed therapist. Visit notes that document patient education without specifying what was taught, what technique or skill was demonstrated, and what the patient’s response was do not establish skilled service. Visit notes that document “patient performed exercises with good tolerance” without specifying what exercises were performed, at what intensity, and what the clinical rationale for the specific program is do not establish the skilled nature of the service being provided.
OASIS accuracy is an audit domain with both compliance and financial dimensions that are inseparably linked. OASIS items that determine the PDGM clinical grouping and functional impairment level — items M1810 through M1860 covering current functional status in grooming, upper and lower body dressing, bathing, toilet transfers, and locomotion — directly affect episode payment. Systematic underscoring of these items — documenting better functional status than the patient actually demonstrates — produces lower PDGM payments than the patient’s actual clinical status would generate. Systematic overscoring — documenting worse functional status than clinical observation supports — produces higher payments that may constitute upcoding with false claims implications. OASIS accuracy audits compare documented functional status to the clinical observations documented in visit notes to identify discrepancies that suggest scoring drift in either direction.
Goal documentation and outcome measurement deserve specific audit attention because they form the clinical narrative framework within which skilled services are justified and evaluated. Goals that are not specific, measurable, achievable, relevant, and time-bound do not provide the compliance documentation framework that home health requires. Goals documented at start of care that never appear again in subsequent visit notes — where visit content has no evident connection to the documented goals — suggest that the plan of care exists as a compliance document rather than a genuine clinical road map. Audits that examine the alignment between documented goals and the specific content of visit notes identify the clinical documentation coherence failures that surveyors find most concerning.
Clinician signature and authentication requirements are a technical documentation compliance area that internal audits should verify routinely. CMS requires that all clinical documentation be authenticated by the clinician who provided the service within specific timeframes, and that authenticated documentation bear the clinician’s full name, credentials, and date of authentication. Late authentication — documentation authenticated after the required timeframe — is both a compliance risk and a clinical quality concern, because documentation completed days after the visit from memory is less accurate than documentation completed contemporaneously. Audit tracking of authentication timeliness by clinician identifies patterns of late documentation that require operational intervention.
Care plan compliance — whether visit content aligns with the authorized plan of care in terms of frequency, duration, and discipline-specific intervention focus — is an audit element that protects agencies from both LUPA risk and the documentation inconsistency between authorized services and delivered services that triggers additional scrutiny. Audits examining whether the visit frequency actually delivered matches the plan of care frequency authorized, whether discipline-specific services are being provided within the scope specified in the care plan, and whether plan of care modifications are documented with appropriate physician authorization identify compliance gaps that are operationally correctable when identified early.
The most important element of any audit program is not the audit itself but the response to findings. Audit findings that are documented, presented to clinical leadership, translated into specific staff education, incorporated into ongoing monitoring, and tracked for improvement over subsequent audit cycles produce quality improvement. Audit findings that are documented but not systematically acted upon produce paper compliance without practice improvement. Building the operational loop from audit finding to educational response to monitored improvement to validated correction is what distinguishes documentation audit programs that actually improve quality from those that exist primarily to demonstrate QAPI compliance to surveyors.
Humane Care Therapy Inc. incorporates documentation quality monitoring into our quality assurance process for all deployed clinicians, and we share audit-informed insights with partner agencies as part of our quality partnership approach. Contact us at (281) 619-3771 or visit humanecaretherapy.com.


