
A Practical Guide for Agencies Integrating Telehealth Into Home Health Practice While Maintaining Clinical and Compliance Standards
Telehealth in home health therapy occupies a position that is simultaneously promising and frequently misunderstood — promising because the technology genuinely enables clinical interactions that extend reach and improve care coordination between in-person visits, and misunderstood because the enthusiasm for telehealth efficiency has in some contexts outpaced honest assessment of what telehealth can and cannot appropriately accomplish in the clinical context of skilled home health therapy. Building a telehealth program that captures the genuine value of remote clinical interaction without creating the clinical quality and billing compliance risks that inappropriate telehealth use generates requires a clear-eyed understanding of both dimensions.
The regulatory framework for telehealth in home health has evolved significantly since the COVID-19 public health emergency, which triggered temporary regulatory flexibilities that expanded telehealth coverage dramatically for the duration of the emergency period. As these flexibilities have been selectively extended, modified, or allowed to expire, the current regulatory landscape requires specific attention to what CMS allows for telehealth in home health, what constitutes a telehealth visit versus a communication technology-based service (CTBS), and which telehealth interactions can support billing claims versus those that represent value-added services delivered outside the billable service framework.
Communication technology-based services — brief virtual check-ins with patients and caregivers that supplement in-person home health visits — are specifically recognized by CMS and can be billed under certain circumstances when conducted by specific clinician types. These brief virtual check-ins are distinct from full telehealth visits that substitute for in-person clinical encounters, and understanding the distinction is essential for billing compliance. A five-minute video call to review the patient’s home exercise program between scheduled in-person visits is a different clinical and billing event than a full 45-minute telehealth session that is claimed as equivalent to an in-person skilled therapy visit.
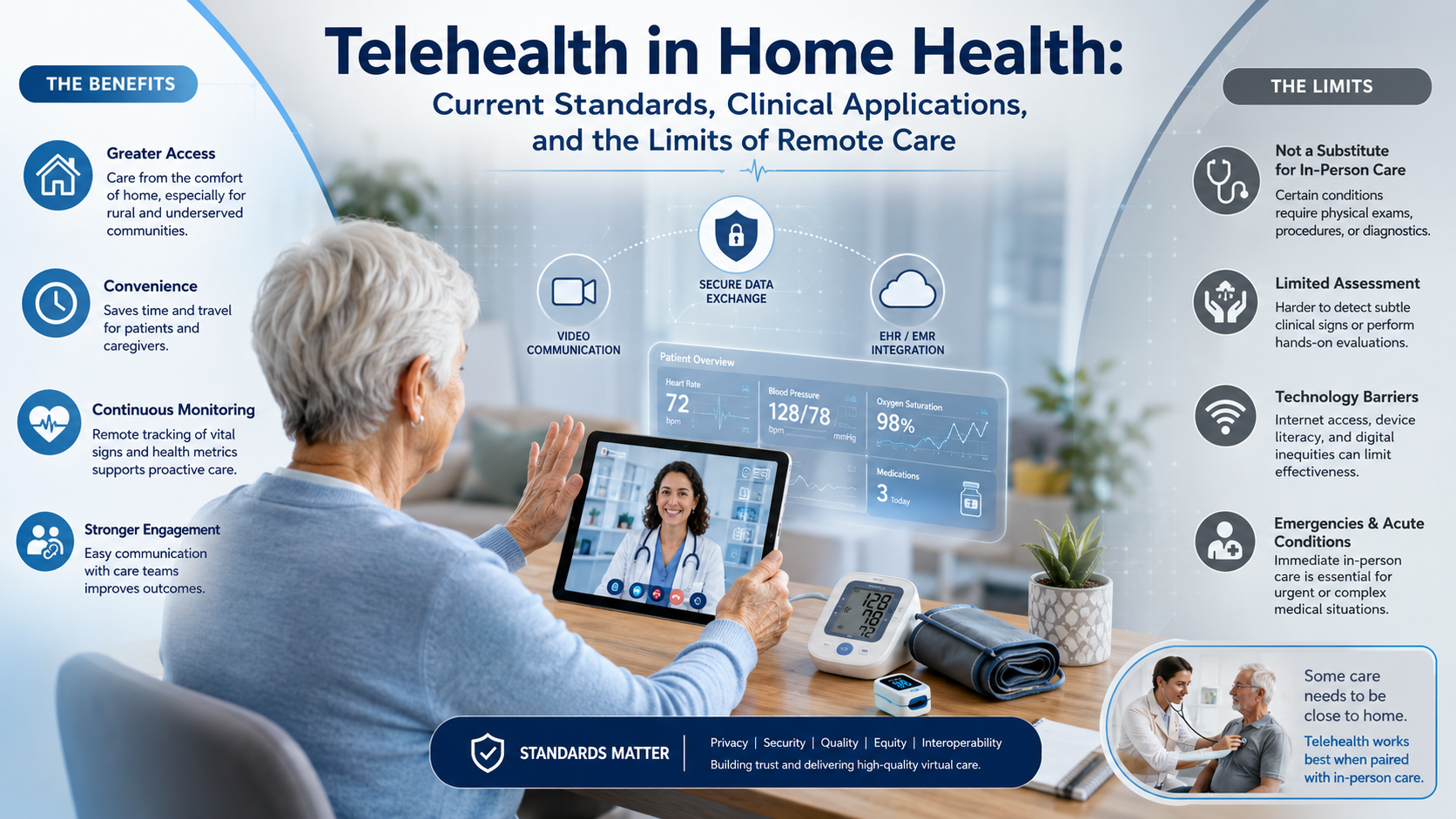
The clinical question of what telehealth can and cannot accomplish in home health therapy is foundational to building a program with integrity. Telehealth interactions can effectively accomplish patient and caregiver education on condition management, home program review and coaching, care coordination communication, motivational check-ins that support program adherence, early identification of clinical concerns that may warrant an in-person visit or physician notification, and communication with the multidisciplinary care team around care planning. These are genuine clinical contributions that extend the clinical team’s reach and impact between visits.
Telehealth interactions cannot accomplish what requires physical presence: hands-on therapeutic manipulation, manual techniques, accurate tactile assessment of tissue quality and joint integrity, clinical observation of gait patterns in the actual home environment with its specific floor surfaces and spatial dimensions, functional assessment that requires the patient to actually perform home tasks, or the safety assessment of the home environment that determines what modifications are needed. Agencies that claim telehealth sessions as substitutes for in-person skilled therapy visits when the clinical content of those sessions cannot be accomplished without physical presence are creating both clinical quality and billing compliance problems that expose them to claim denial and audit risk.
Patient selection for telehealth is as important as session content design. Patients with significant cognitive impairment may not be able to effectively participate in telehealth sessions that require following verbal or visual instructions without in-person support. Patients with technology barriers — no smartphone, tablet, or computer access; no reliable internet connection; or inadequate technological literacy — cannot effectively participate in video telehealth regardless of clinical appropriateness. Patients whose care needs require physical presence at every visit have no appropriate telehealth substitution regardless of technology access. Telehealth is most appropriate for patients who are clinically stable, who have adequate technology access and literacy, who have a motivated caregiver who can support telehealth participation if needed, and whose specific between-visit care need is addressable through coaching, education, or monitoring rather than hands-on intervention.
Consent and documentation requirements for telehealth in home health are specific and must be addressed before telehealth services are delivered. Patient consent to telehealth must be obtained and documented, including confirmation that the patient understands they are participating in a telehealth visit rather than an in-person visit and their right to choose in-person services. Documentation of telehealth visits must specify the modality used, the patient location, the clinician location, the clinical content delivered, and the clinical assessment accomplished — at the same level of specificity that in-person documentation requires. Generic documentation that would not be accepted for an in-person visit is equally unacceptable for a telehealth visit.
Technology platform requirements for clinical telehealth in home health include HIPAA compliance of the video platform used, audio and video quality adequate for clinical observation, reliability across the internet connections available to the patient population served, and ease of use appropriate for the patient demographic. Many home health patients are elderly adults with varying levels of technological familiarity — platform selection should be made with this population in mind rather than defaulting to the platform most familiar to clinical staff. Telephone-only visits without video capability have more limited clinical utility than video visits but may be appropriate for specific communication-focused services when video access is not available.
Integrating telehealth with in-person care to produce a care model that uses each modality for the clinical interactions it is best suited for — rather than simply adding telehealth visits to existing schedules or substituting telehealth for in-person visits to reduce cost — requires clinical program design that begins with the specific clinical goals the program is trying to achieve. What between-visit clinical needs currently go unaddressed that telehealth could address? What clinical concerns generate unnecessary in-person visits that a telehealth check-in could appropriately triage? What patient education content is currently compressed into in-person visits because no between-visit delivery mechanism exists, and would benefit from a dedicated telehealth education session? These clinical design questions produce a telehealth program that adds clinical value rather than one that adds administrative complexity without clinical return.
Humane Care Therapy Inc. provides clinicians who are comfortable integrating telehealth into home health practice within the clinical and regulatory framework that maintains both quality and compliance. Contact us at (281) 619-3771 or visit humanecaretherapy.com.


